

How To Protect Against COVID-19
Coronaviruses are a large group of viruses that cause many common human and animal infections. In humans, coronaviruses typically cause mild respiratory infections. Estimated 10–30% of all upper respiratory tract infections are caused by coronaviruses. Coronaviruses are one of the main causes of the common cold. Coronaviruses are highly adaptable and known to undergo host-switching. Once adapted to the human host, coronaviruses can transmit between humans. During the last decade, new coronaviruses have been evolved to cause potentially life-threatening respiratory diseases. These include severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS) coronaviruses. The SARS pandemic in the early 2000s lasted about nine months, affected over 8,000 people in 29 world regions, and caused a fatality in almost 10% of cases. MERS mainly stayed in Arabian Peninsula infecting approximately 2,400 people with a fatality rate of nearly 35%.
The fatality rate of typical influenza viruses is much lower, reaching a maximum of about 0.2% in people over 75 years old; but, due to its high occurrence, it has contributed to higher infection rates.
The coronavirus SARS-CoV-2 was identified in late 2019; and the disease it causes is called COVID-19.
Although the full characteristics of COVID-19 are still being investigated, based on the current information, the illness is considered a serious health threat. Human coronaviruses cause infections of the nose, throat, and lungs. They are most commonly spread from an infected person through respiratory droplets generated by coughing or sneezing; prolonged personal contact, such as touching or shaking hands; touching something with the virus on it, then touching the mouth, nose or eyes before washing hands; and the risk for getting COVID-19 may be increased for travelers.
It is not certain how long COVID-19 survives on surfaces, but it appears to behave like other coronaviruses. Preliminary information on COVID-19 suggests that the virus may persist on surfaces for a few hours or up to several days depending on different conditions, such as temperature, type of surface, the humidity of the environment. In general, surfaces frequently touched with hands are most likely to be contaminated, including tables, handrails, doorknobs, electronics, countertops, light switches, faucet handles, cabinet handles, and elevator buttons.
There is an increased risk of infection with more severe complications amongst those aged 65 and over; with compromised immune systems; and those with underlying medical conditions such as obesity, diabetes, or hypertension.
Because COVID-19 is a new disease, there's a lot to learn about its long term effects on health as well as that how it affects pregnant women. Currently, there is no evidence to suggest that pregnant women are at a greater risk for more serious outcomes related to COVID-19 or that their developing child could be negatively affected by COVID-19.
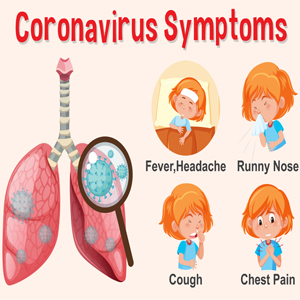
COVID-19 Signs and symptoms:
Based on the current data, fever, dry cough along with flu-like symptoms are the most common symptom of COVID-19. In some cases, it has been reported that patients may experience early eye-related symptoms, such as conjunctivitis (pink eye) and eye discharge. Also; Gastrointestinal symptoms such as loss of appetite or diarrhea in addition to—or in rare cases instead of—initial respiratory symptoms are observed.
Other symptoms including loss of sense of smell and taste are also commonly reported. Although the loss of sense of smell and taste can occur with other viral respiratory diseases such as the common cold or influenza, these are thought to be much more common in COVID-19.
The severity of the COVID-19 is related to increased blood clotting and vascular complications throughout the body. More importantly, it appears that the infection with the Covid-19 causes excessive clotting in the tiny capillaries in the lungs where oxygen and carbon dioxide exchange takes place. Clot formation in these tiny blood vessels impairs the lungs’ ability to oxygenate the blood. Clotting tendency also is considered the reason for the too high incidence of ischemic strokes in younger people with COVID-19 who do not have traditional stroke risk factors. Accordingly, anti-coagulant use has become a standard of care recommended by most expert panels.
Skin manifestations such as rashes, plaque-like lesions, and painful red or purple lesions on the fingers or toes are increasingly being observed in the cases of COVID-19. It is suggested that whether these could be due to inflammatory effects of the SARS-CoV-2 virus, or secondary effects of blood clotting which damages the delicate blood vessels of the skin.
Although further research is necessary to determine the cause of the skin symptoms, appearing of unusual rash or skin problems should be mentioned to the healthcare providers, especially if it is accompanied by other potential COVID-19 symptoms.
In older individuals and those with pre-existing conditions, rapid progression of the disease to acute respiratory distress syndrome (ARDS) and death is most commonly observed.

How to Protect Against Covid-19?
Avoiding contact with infected individuals is the most effective strategy to protect yourself from COVID-19. Since at its beginning the infection does not show symptoms maintaining distance of at least 6 feet or 2 meters from others, limiting activity outside the home as much as possible can help limit the spread of infection.
In general avoiding non-essential travels helps decrease the infection outbreaks including measles, influenza, SARS, and many others. Therefore, avoiding air travel is a reasonable precaution for reducing the risk of viral infections particularly for vulnerable individuals.
Frequent hand washing is an important strategy for protecting against all types of infectious diseases. Studies have further demonstrated the strategic use of alcohol-based surface disinfectants and hand sanitizers can reduce viral spread by 85–94%.
An optimal functioning immune system is vital for defending against all types of infections, from mild colds to dangerous influenza and life-threatening pneumonia. A nutrient-dense diet, adequate sleep, physical activity, and stress management all can help maintain a healthy immune function.
University researchers found that SARS-CoV-2 aerosols were detectable for up to three hours. The virus was detectable on cardboard for up to 24 hours and up to three days on plastic and stainless steel. Proper cleaning and disinfecting agents eliminate the virus and help limit the spread of infectious diseases caused by coronaviruses. A study published on February 6th, 2020 found that coronaviruses on inanimate surfaces can be inactivated within one minute through disinfection with 62%‒71% ethanol, 0.5% hydrogen peroxide, or 0.1% sodium hypochlorite (eg, bleach).
Wearing a face mask in public is recommended by the CDC and other health organizations. Face mask helps prevent the spread of infection by infected individuals by reducing the dispersion of respiratory droplets into the environment. This is particularly important because many people infected with SARS-CoV-2 show no or mild symptoms and may not realize they have it. Public health organizations recommend to preferably use cloth facemasks made of high-quality, high-thread-count woven cotton and reserve surgical masks and N95 respirator masks for healthcare workers. Masks should not be used as a substitute for social distancing.
Detection of IgG antibodies to SARS-CoV-2 suggests that a person was likely exposed to the virus at some point in the past. However; the accuracy of the test depends on some factors including but not limited to its sensitivity, specificity, and the existence of the disease in the community.
At this time, the presence of IgG antibodies to SARS-CoV-2 is not known to indicate immune protection. More research is underway to clarify this critical question.

SARS-CoV-2/COVID-19 Vaccine Research
Many experts suggest that COVID-19 remains a global health concern until a safe and effective vaccine has been developed and administered to much of the world’s population. Developing any kind of vaccine is time-consuming and must go through long enough trials for safety and efficacy. Vaccines must perform outstanding safety and efficacy to be administered to most of the people.
There are several general methods and types of vaccines being studied against COVID-19 including:
Live attenuated or inactivated virus vaccines: aimed to use modified variants of the SARS-CoV-2 virus that do not cause disease but can cause the immune system to create a defense against future SARS-CoV-2 exposures. Many familiar vaccines such as influenza and measles vaccines are of this type.
Viral vector vaccines will incorporate SARS-CoV-2 genes into a different, non-pathogenic virus. Administering such a vaccine does not cause disease but it creates an immune defense against SARS-CoV-2 upon future exposure.
Subunit vaccines deliver specific proteins or antigens unique to the SARS-CoV-2 virus that can prime the immune system to respond against a future SARS-CoV-2 infection. These types of vaccines are used against hepatitis B and whooping cough.
Nucleic acid vaccines are utilizing a new technology that delivers the genetic material (DNA and/or RNA) containing codes for the viral antigens, then the body's cells use theses genetic material to manufacture the antigens, alerting the immune system to identify future exposures to SARS-CoV-2. No vaccines of this type have been approved as of June 2020.
As of mid-June 2020, there are at least three vaccine candidates for phase 3 trials which are set to start during summer into the fall.
long-term clinical trials are essential to ensure that any vaccine candidate is not only effective in preventing its target disease, but also safe. Phase 3 vaccine trials are a long time process because vaccinated subjects must be followed-up for many months to conclude whether they got sick when exposed to the circulating virus, also to follow subjects for a long time to find out how long the generated immunity by the vaccine lasts. One potential challenge is that vaccines that are shown to work in younger individuals may not provide the same degree of immunity to older adults.
If all goes well most experts expect that the first vaccine(s) will become available in mid-to-late 2021 at the earliest, and vaccinating the world population would extend beyond 2021.
Basic Integrative Medicine Options:
There are many integrative therapies with well known antiviral and immune-modulating benefits. An integrative approach is not specifically for severe viral infections however it may provide reasonable support for the respiratory tract and/or immune system.
It is shown that vitamin C, both before and soon after the onset of symptoms of upper respiratory tract infections, may help ease symptom and reduce the duration of illness
N-acetylcysteine (NAC) is an amino acid compound with mucolytic properties often used for respiratory conditions. Supplementing with NAC helped shorten the duration of intensive care unit (ICU) stay compared with control among patients with ARDS. Based on some positive observational information during late 2019 and early 2020, some Chinese institutions have initiated using NAC as part of the standard management of patients in the hospital setting. Some researchers have suggested NAC could help support the health of mucous-producing cells lining the respiratory tract in some patients suffering from SARS-type viral respiratory conditions due to its potent antioxidant and mucolytic functions.
Lactoferrin has shown antibacterial, antiviral, and antifungal properties. It helps to activate the antiviral cytokines interferon (IFN)-α/β and increase natural killer (NK) cell activity and Th1 cytokine responses. It is suggested that taking lactoferrin may help reduce the frequency and severity of common respiratory tract viral infections, like colds and flu. Research found that the gene encoding lactoferrin was highly upregulated in patients affected by SARS suggesting that it plays a role in the innate immune response to the infection. Later, a follow-up study suggested that lactoferrin interfered with the ability of the 2003 SARS virus from compromising the functional and structural integrity of host cells.
Selenium is an important antioxidant, with anti-inflammatory, and antiviral activities in the body. Selenium deficiency is associated with an increased risk of viral infection. Low selenium levels found to be associated with increased mortality in HIV patients.
Probiotic species of Bifidobacterium and Lactobacillus play a role in supporting the host’s immune response and may help reduce the frequency, severity, and duration of viral respiratory tract infections such as influenza.
Low levels of vitamin D contribute to higher risks of developing pneumonia. An analysis of randomized controlled trial data found vitamin D supplementation has helped to reduced the risk of respiratory infections by over 40%. Vitamin D helps increase antimicrobial immune activity; and vitamin D deficiency is associated with fewer immune cells in the blood, increasing susceptibility to infection. Vitamin D is an immune modulator by playing a role in stimulating innate immune activity and regulating inflammation.
Related articles:
How To Treat Cold Sores With Natural Medicine
Natural Solutions to Quick Recovery from Common Cold
Medicinal Mushrooms and their Immune boosting power
How to Improve Immunity Against Coronavirus
Articles and products featured by Health Palace are collected from a variety of sources and are provided as a service by Health Palace. These newsletters, while of potential interest to readers, do not necessarily represent the opinions nor constitute the advice of Health Palace. Presented materials are only for information purposes and do not intent to treat, cure, or prevent any disease.
References:
1.WHO. World Health Organization. Novel Coronavirus (2019-nCoV).https://www.who.int/emergencies/diseases/novel-cor... Published 2020. Accessed 1/29/2020.
2.CDC. Centers for Disease Control and Prevention. 2019 Novel Coronavirus (2019-nCoV), Wuhan, China. https://www.cdc.gov/coronavirus/2019-ncov/summary.... Published 2020. Updated 1/28/2020. Accessed 1/29/2020
3.Li G, Fan Y, Lai Y, et al. Coronavirus infections and immune responses. Journal of medical virology. 2020;92(4):424-432.
4.Azhar EI, Hui DSC, Memish ZAy, Drosten C, Zumla A. The Middle East Respiratory Syndrome (MERS). Infectious disease clinics of North America. 2019;33(4):891-905.
5.Paules CI, Marston HD, Fauci AS. Coronavirus Infections-More Than Just the Common Cold. JAMA. 2020:10.1001/jama.2020.0757.
6.Hui DSC, Zumla A. Severe Acute Respiratory Syndrome: Historical, Epidemiologic, and Clinical Features. Infectious disease clinics of North America. 2019;33(4):869-889.
7.Li B, Yang J, Zhao F, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin Res Cardiol. 2020.
8.Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. Journal of medical virology. 2020;92(4):441-447.
9.Killerby ME, Biggs HM, Midgley CM, Gerber SI, Watson JT. Middle East Respiratory Syndrome Coronavirus Transmission. Emerg Infect Dis. 2020;26(2):191-198.
10.Iuliano AD, Roguski KM, Chang HH, et al. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2018;391(10127):1285-1300.
11.Judson SD, Munster VJ. Nosocomial Transmission of Emerging Viruses via Aerosol-Generating Medical Procedures. Viruses. 2019;11(10).
12.Wu P, Duan F, Luo C, et al. Characteristics of Ocular Findings of Patients With Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmology. 2020.
13.Pan L, Mu M, Yang P, et al. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. The American journal of gastroenterology. 2020;115(5):766-773.
14.Xiao F, Tang M, Zheng X, et al. Evidence for gastrointestinal infection of SARS-CoV-2. medRxiv. 2020:2020.2002.2017.20023721.
15.Lechien JR, Chiesa-Estomba CM, De Siati DR, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. European Archives of Oto-Rhino-Laryngology. 2020:1.
16.Yan CH, Faraji F, Prajapati DP, Boone CE, DeConde AS. Association of chemosensory dysfunction and Covid-19 in patients presenting with influenza-like symptoms. International forum of allergy & rhinology. 2020;n/a(n/a).
17.Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up. Journal of the American College of Cardiology. 2020:27284.
18.Carsana L, Sonzogni A, Nasr A, et al. Pulmonary post-mortem findings in a large series of COVID-19 cases from Northern Italy. medRxiv. 2020:2020.2004.2019.20054262.
19.Fogarty H, Townsend L, Ni Cheallaigh C, et al. COVID-19 Coagulopathy in Caucasian patients. Br J Haematol. 2020.
20.Lee SG, Fralick M, Sholzberg M. Coagulopathy associated with COVID-19. CMAJ. 2020.
21.Lodigiani C, Iapichino G, Carenzo L, et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. 2020;191:9-14.
22.Rabin RC. What Is ‘Covid Toe’? Maybe a Strange Sign of Coronavirus Infection. The New York Times. https://www.nytimes.com/2020/05/01/health/coronav... Updated 05/05/2020. Accessed 05/18/2020.
23.Dolhnikoff M, Duarte-Neto AN, de Almeida Monteiro RA, et al. Pathological evidence of pulmonary thrombotic phenomena in severe COVID-19. J Thromb Haemost. 2020.
24.Wu C, Chen X, Cai Y, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020.
25.Corman VM, Muth D, Niemeyer D, Drosten C. Hosts and Sources of Endemic Human Coronaviruses. Advances in virus research. 2018;100:163-188.
26.La Rosa G, Fratini M, Della Libera S, Iaconelli M, Muscillo M. Viral infections acquired indoors through airborne, droplet or contact transmission. Annali dell'Istituto superiore di sanita. 2013;49(2):124-132.
27.Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and its inactivation with biocidal agents. The Journal of hospital infection. 2020:S0195-6701(0120)30046-30043.
28.van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. The New England journal of medicine. 2020;382(16):1564-1567.
29.CDC. Centers for Disease Control and Prevention. Preventing COVID-19 Spread in Communities. https://www.cdc.gov/coronavirus/2019-ncov/communi... Published 2020. Updated 3/10/2020. Accessed 5/7/2020.
30.CDC. Centers for Disease Control and Prevention. Travelers' Health: China Traveler View. https://wwwnc.cdc.gov/travel/destinations/travele... Published 2020. Updated 1/20/2020. Accessed 1/30/2020.
31.Mangili A, Vindenes T, Gendreau M. Infectious Risks of Air Travel. Microbiol Spectr. 2015;3(5).
32.Kurgat EK, Sexton JD, Garavito F, et al. Impact of a hygiene intervention on virus spread in an office building. Int J Hyg Environ Health. 2019;222(3):479-485.
33.Reynolds KA, Sexton JD, Pivo T, Humphrey K, Leslie RA, Gerba CP. Microbial transmission in an outpatient clinic and impact of an intervention with an ethanol-based disinfectant. American journal of infection control. 2019;47(2):128-132.
34.CDC. Centers for Disease Control and Prevention. Use of Cloth Face Coverings to Help Slow the Spread of COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/prevent... Published 2020. Updated 4/4/2020. Accessed 4/6/2020.
35.Bai Y, Yao L, Wei T, et al. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA. 2020.
36.Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. New England Journal of Medicine. 2020;382(10):970-971.
37.NASEM. Rapid Expert Consultation on SARS-CoV-2 Laboratory Testing for the COVID-19 Pandemic. https://www.nap.edu/read/25775/chapter/1. Published 2020. Accessed 5/8/2020.
38.CDC. Evaluating and Testing Persons for Coronavirus Disease 2019 (COVID-19). https://www.cdc.gov/coronavirus/2019-nCoV/hcp/cli... Published 2020. Updated 3/24/2020. Accessed 5/8/2020.
39.Arevalo-Rodriguez I, Buitrago-Garcia D, Simancas-Racines D, et al. FALSE-NEGATIVE RESULTS OF INITIAL RT-PCR ASSAYS FOR COVID-19: A SYSTEMATIC REVIEW. medRxiv. 2020:2020.2004.2016.20066787.
40.Vaccine Types. Published by U. S. National Institute of Allergy and Infectious Diseases. https://www.niaid.nih.gov/research/vaccine-types Updated 07/01/2019. Accessed 06/10/2020.
41.Holmes B. The time of trials: Waiting for a coronavirus vaccine. Published by Knowable Magazine. https://www.knowablemagazine.org/article/health-d... Updated 05/22/2020. Accessed 06/10/2020.
42.HHS. U.S. Department of Health & Human Services. Vaccine Types. https://www.vaccines.gov/basics/types. Accessed 06/11/2020.
43.Loftus P. Coronavirus Vaccine Candidates’ Pivotal U.S. Testing to Start This Summer. Published by The Wall Street Journal. https://www.wsj.com/articles/coronavirus-vaccine-... Updated 06/10/2020. Accessed 06/10/2020.
44.Mayo Clinic. COVID-19 (coronavirus) vaccine: Get the facts. https://www.mayoclinic.org/diseases-conditions/co... Updated 06/10/2020. Accessed 06/10/2020.
45.Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 Vaccines at Pandemic Speed. New England Journal of Medicine. 2020;382(21):1969-1973.
46.Zapatera B, Prados A, Gomez-Martinez S, Marcos A. Immunonutrition: methodology and applications. Nutr Hosp. 2015;31 Suppl 3:145-154.
47.Gorton HC, Jarvis K. The effectiveness of vitamin C in preventing and relieving the symptoms of virus-induced respiratory infections. Journal of manipulative and physiological therapeutics. 1999;22(8):530-533.
48.Hemilä H, Douglas RM. Vitamin C and acute respiratory infections. The international journal of tuberculosis and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease. 1999;3(9):756-761.
49.Ran L, Zhao W, Wang J, et al. Extra Dose of Vitamin C Based on a Daily Supplementation Shortens the Common Cold: A Meta-Analysis of 9 Randomized Controlled Trials. Biomed Res Int. 2018;2018:1837634.
50.Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. The Cochrane database of systematic reviews. 2013(1):CD000980.
51.Vorilhon P, Arpajou B, Vaillant Roussel H, Merlin É, Pereira B, Cabaillot A. Efficacy of vitamin C for the prevention and treatment of upper respiratory tract infection. A meta-analysis in children. Eur J Clin Pharmacol. 2019;75(3):303-311.
52.Blasi F, Page C, Rossolini GM, et al. The effect of N-acetylcysteine on biofilms: Implications for the treatment of respiratory tract infections. Respiratory medicine. 2016;117:190-197.
53.Kalyuzhin OV. Effect of N-acetylcysteine on mucosal immunity of respiratory tract. Terapevticheskii arkhiv. 2018;90(3):89-95.
54.Samuni Y, Goldstein S, Dean OM, Berk M. The chemistry and biological activities of N-acetylcysteine. Biochim Biophys Acta. 2013;1830(8):4117-4129.
55.Zhang Y, Ding S, Li C, Wang Y, Chen Z, Wang Z. Effects of N-acetylcysteine treatment in acute respiratory distress syndrome: A meta-analysis. Experimental and therapeutic medicine. 2017;14(4):2863-2868.
56.McCarty MF, DiNicolantonio JJ. Nutraceuticals have potential for boosting the type 1 interferon response to RNA viruses including influenza and coronavirus. Progress in cardiovascular diseases. 2020. [Epub ahead of print]
57.Baveye S, Elass E, Mazurier J, Spik G, Legrand D. Lactoferrin: a multifunctional glycoprotein involved in the modulation of the inflammatory process. Clinical chemistry and laboratory medicine: CCLM/FESCC. 1999;37(3):281-286.
58.Malaczewska J, Kaczorek-Lukowska E, Wojcik R, Siwicki AK. Antiviral effects of nisin, lysozyme, lactoferrin and their mixtures against bovine viral diarrhoea virus. BMC Vet Res. 2019;15(1):318.
59.Wakabayashi H, Oda H, Yamauchi K, Abe F. Lactoferrin for prevention of common viral infections. Journal of infection and chemotherapy: official journal of the Japan Society of Chemotherapy. 2014;20(11):666-671.
60.Ishikawa H, Awano N, Fukui T, Sasaki H, Kyuwa S. The protective effects of lactoferrin against murine norovirus infection through inhibition of both viral attachment and replication. Biochemical and biophysical research communications. 2013;434(4):791-796.
61.Vitetta L, Coulson S, Beck SL, Gramotnev H, Du S, Lewis S. The clinical efficacy of a bovine lactoferrin/whey protein Ig-rich fraction (Lf/IgF) for the common cold: a double blind randomized study. Complementary therapies in medicine. 2013;21(3):164-171.
62.Reghunathan R, Jayapal M, Hsu LY, et al. Expression profile of immune response genes in patients with Severe Acute Respiratory Syndrome. BMC immunology. 2005;6:2.
63.Lang J, Yang N, Deng J, et al. Inhibition of SARS pseudovirus cell entry by lactoferrin binding to heparan sulfate proteoglycans. PLoS One. 2011;6(8):e23710.
64.Wrobel JK, Power R, Toborek M. Biological activity of selenium: Revisited. IUBMB Life. 2016;68(2):97-105.
65.Jespersen L, Tarnow I, Eskesen D, et al. Effect of Lactobacillus paracasei subsp. paracasei, L. casei 431 on immune response to influenza vaccination and upper respiratory tract infections in healthy adult volunteers: a randomized, double-blind, placebo-controlled, parallel-group study. Am J Clin Nutr. 2015;101(6):1188-1196.
66.Waki N, Matsumoto M, Fukui Y, Suganuma H. Effects of probiotic Lactobacillus brevis KB290 on incidence of influenza infection among schoolchildren: an open-label pilot study. Lett Appl Microbiol. 2014;59(6):565-571.
67.Maruyama M, Abe R, Shimono T, Iwabuchi N, Abe F, Xiao JZ. The effects of non-viable Lactobacillus on immune function in the elderly: a randomised, double-blind, placebo-controlled study. Int J Food Sci Nutr. 2016;67(1):67-73.
68.Muzembo BA, Ngatu NR, Januka K, et al. Selenium supplementation in HIV-infected individuals: A systematic review of randomized controlled trials. Clinical nutrition ESPEN. 2019;34:1-7.
69.Harthill M. Review: micronutrient selenium deficiency influences evolution of some viral infectious diseases. Biol Trace Elem Res. 2011;143(3):1325-1336.
70.Leow L, Simpson T, Cursons R, Karalus N, Hancox RJ. Vitamin D, innate immunity and outcomes in community acquired pneumonia. Respirology (Carlton, Vic.). May 2011;16(4):611-616.
71.Lin R. Crosstalk between Vitamin D Metabolism, VDR Signalling, and Innate Immunity. BioMed Research International. 2016;2016:1375858.
72.Quraishi SA, Bittner EA, Christopher KB, Camargo CA, Jr. Vitamin D status and community-acquired pneumonia: results from the third National Health and Nutrition Examination Survey. PloS one. 2013;8(11):e81120.
73.Youssef DA, Ranasinghe T, Grant WB, Peiris AN. Vitamin D's potential to reduce the risk of hospital-acquired infections. Dermatoendocrinol. Apr 1 2012;4(2):167-175.
74.Cannell JJ, Hollis BW. Use of vitamin D in clinical practice. Altern Med Rev. 2008;13(1):6-20.
75.Cannell JJ, Vieth R, Umhau JC, et al. Epidemic influenza and vitamin D. Epidemiol Infect. 2006;134(6):1129-40.
Recent Posts
-

Maintain A Healthy Heart Rhythm With Integrative Medicine
Maintain A Healthy Heart Rhythm With Integrative Medicine;Usually, abnormal heart rate or arrhythmi …4th Feb 2021 -

How To Protect Against COVID-19
Coronaviruses are a large group of viruses that cause many common human and animal infections. In hu …30th Jun 2020 -

How to Prevent Gallstones from Forming? | Natural Supplements for Gallstones
How To Prevent Gallstone Formation?Gallstones are hard deposits made of cholesterol or bilirubin f …4th Mar 2020